


by Monica Mollica
In the past, anabolic steroids were used primarily by athletes in order to boots physical performance. However, today anabolic steroids are also common among non-athletes, who use them with the goal to improve their physique and appearance. It was recently estimated that among Americans aged 13-50 years, 2.9 to 4.0 million have used anabolic steroids.[1] Within this group, roughly 1 million may have experienced anabolic steroid dependence.[1]
Most of these folks have gone down this pathway blindly, obviously without physician supervision, using underground black market resources and products. Not only is non-medically supervised use of anabolic steroids per see potentially dangerous, but the purity of underground products is highly speculative, which adds additional health risks. Also, because of the common practice of “stacking”, which is use of two or more anabolic steroids (often androgens) in progressively increasing doses in cycles lasting for different durations of time, it is hard to predict the cumulative potential health consequences. Also, most anabolic steroids are synthetic man-made compounds that are not natural to the body. This is in contrast to testosterone, which is naturally produced by the body and necessary, in the physiological range, for health and wellbeing. Anabolic steroids are not.
For those who have chosen to use anabolic steroids, this article will outline ways to restore the HPG-axis (Hypothalamic-Pituitary-Gonadal axis).
Side effects
Anabolic steroid use come with side effects, including liver and heart damage (cardiomyopathy), thickening of the blood (polycythemia), deleterious changes in cholesterol and blood fat profiles (dyslipidemia), high blood pressure (hypertension), depression, gynecomastia (aka “bitch tits”), testicular shrinkage, erectile and sexual dysfunction, and infertility.[2-9] Some side effects, such as erectile and sexual dysfunction and depression, usually don’t show up until after a cycle has been completed and testosterone levels have dropped to below normal (see below).[8]
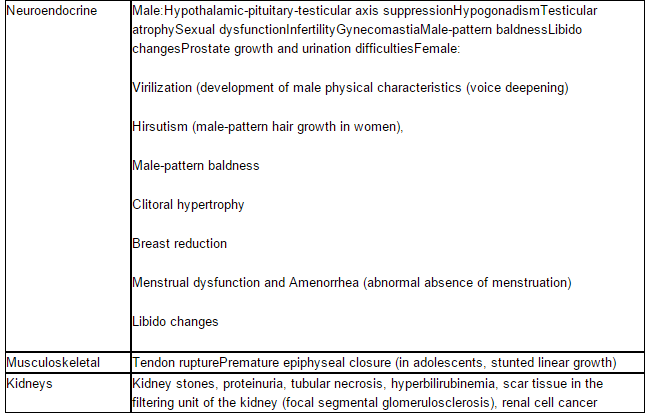
The negative effects of anabolic steroids on the heart and cardiovascular system are especially well-documented.[5, 10-19] While some effects on the heart may be reversible, others (like direct injury to heart and blood vessel cells and fibrosis) are not and thus may cause permanent deterioration in heart function.[16] In addition to detrimental alterations in cardiac structure and function [11-14], anabolic steroids cause insulin resistance and negative alterations in lipid profiles (reduced HDL and apoA, and increased triglycerides, LDL, C-reactive protein and homocysteine), which speed up development of atherosclerosis and heart disease.[5, 12, 16] Table 1 lists the most common side effects of anabolic steroids
Table 1. Possible anabolic steroid use side effects.[16, 17]

Anabolic steroid-induced hypogonadism (ASIH)
As mentioned, anabolic steroids are usually taken in cycles. Cycling refers to the intermittent use of anabolic steroids where a cycle is followed by a drug holiday. The practice of “cycling” is based on the notion that drug holidays prevent desensitization to large doses of androgen (even though this concept remains to be proven scientifically).[20]
Administration of anabolic steroids (including therapeutic doses of testosterone [21, 22]) suppresses pituitary LH and FSH secretion, which in turn reduces testicular size, testosterone production and sperm production.[6, 8, 22-25] After a cycle of anabolic steroid use, the recovery of the hypothalamic-pituitary-gonadal (HPG) axis may take months to years, depending on the dose and duration of prior androgen use.[5, 6, 8]
During this period, testosterone levels may fall to very low levels as the effects of the supplemented testosterone wear off and the HPT axis has yet not recovered, known as anabolic steroid-induced hypogonadism.[6, 24, 26, 27] It is not uncommon for male users to experience testosterone levels below 200 ng/dL despite abstinence from anabolic steroids for up to 4 years.[8, 28] Sometimes testosterone levels may drop as low as 20-50 ng/dL [24, 25], which is in the female range. Anabolic steroid-induced hypogonadism is a potentially under-recognized cause of hypogonadism in young men.[25]
During this post-cycle period, users may experience troublesome symptoms of androgen deficiency, including loss of sexual desire and sexual function, depressed mood, and hot flushes. Some find these withdrawal symptoms so difficult to tolerate that they go back on another cycle before their HPT axis has recovered, or may seek other psychoactive drugs, thus creating a vicious cycle of anabolic steroid use, withdrawal symptoms, and dependence [29-33], also known as “hooked-on-hormones” syndrome.[34]
Anabolic steroid induced hypogonadism is typically secondary hypogonadism, caused by a deficiency of LH due to a shutdown of the HPG-axis. In contrast, primary hypogonadism is caused by testicular insensitivity to LH. It should be noted that post-cycle therapy only works for secondary hypogonadism. Some anabolic steroids (for example nandrolone decanoate) may potentially cause testicular toxicity when used in high doses for a long time.[35] Whether this may cause primary hypogonadism is not known, but possible. In such cases, none of the post-cycle therapies will help. The only solution would be lifelong medical testosterone replacement therapy.
Post Cycle Therapy (PCT)
Although the anabolic steroid induced suppression of the HPG axis usually recovers spontaneously when use of anabolic steroid is discontinued, this may take several years, and sometimes spontaneous recovery does not always take place.[36] The duration of suppression and the resultant symptomatic hypogonadism is highly variable and due to multiple factors, including differences in anabolic steroid preparations and amounts used, as well as duration of use. Younger men may have a more ‘‘elastic axis’’ capable of recovering GnRH pulsation and gonadotropin (LH and FAS) secretion faster and more completely than older anabolic steroid users.[37] It is possible that shorter durations, lower doses, younger ages, and higher baseline testosterone levels at are associated with a faster recovery of HPG-axis function after anabolic steroid use.[26]
Post cycle therapy helps to restore natural function of the hypothalamic-pituitary-gonadal axis (HPG axis) after it has been suppressed by the use of self-prescribed anabolic steroids. It is important to regain pituitary and testicular function as soon as possible in order to prevent hypogonadism-induced health consequences, such as loss of muscle and bone mineral mass, sexual and reproductive dysfunction, and depression, as well as to promote healthy aging.
There is currently no FDA approved drug to restore HPG axis function after anabolic steroid use. Treatment therefore involves using various dosages of hCG and clomid, often in combination with the tamoxifen (a selective estrogen receptor inhibitor) or arimidex (an aromatase inhibitor). A potential new strategy is LH/FSH priming by a GnRH challenge (the triptorelin test) as a way to kick-start the HPG-axis (more info below).
hCG (Human Chorionic Gonadotropin)
hCG is an LH analogue (i.e. it acts like LH) and thus stimulates testicular production of testosterone, and increases both intra-testicular testosterone and blood testosterone levels. Often hCG is stacked with anabolic steroids when tapering down off a cycle in an attempt to restore testicular size and testosterone-producing capacity and to maintain some of the anabolic effects associated with androgens. However, it should be underscored that hCG, while providing the testicles with an “LH stimulus”, postpones recovery of the HPG axis as acts like an LH supplement and does not stimulate the HPG-axis to secrete LH or FSH. Thus, contrary to popular belief, hCG does not “restore” the function of the HPG axis, it merely give an external stimulus to the testicles to produce testosterone.
Despite acute elevations in testosterone after 1 injection of hCG in androgen users just coming off of a cycle [38], it appears administration of hCG (5,000 IU) 3 times per week for at least a couple of weeks may be needed to reach and maintain normal testosterone levels.[39] The efficacy of hCG was confirmed in a case-report of a young competitive bodybuilder who developed profound symptomatic hypogonadotrophic hypogonadism due to use of anabolic steroids. [24] With a baseline testosterone level of 245 ng/dL (8.5 nmol/L) and impotence he was given injections of hCG for 3 months to stimulate testicular function; 10 000 IU im weekly the first month, 5000 IU weekly the second month, and 2500 units the last month. Within a week of starting treatment, libido had greatly improved and spontaneous nocturnal ejaculations occurred. Testosterone levels and potency returned to normal over the three months of treatment.[24]
In a previous article we described two studies showing that combining testosterone replacement therapy with hCG helps preserving fertility in hypogonadal men on testosterone treatment.[40, 41. Based on this research, users of anabolic steroids may be tempted to use hCG during their cycles as a way to avoid deterioration in spermatogenesis (sperm production) and sperm quality. A study in power athletes found a significant positive correlation between hCG dose during the cycle and the relative amount of abnormal sperma, i.e. use of higher hCG dosages during a cycle was related to deterioration in sperm quality.[42] However, the concomitant use of hCG and massive doses of anabolic steroids did help maintain sperm production, and thereby could help prevent or reduce the degree of testicular shrinkage during a cycle.[42]
hMG (Human Menopausal Gonadotropin, aka menotropin)
There is some speculation (mostly non-scientific) over the potential utility of hMG as part of PCT. hCG is primarily used as a source of LH to stimulate testosterone secretion by Leydig cells, whereas hMG primarily is used as a source of FSH [43], even though hMG also has some LH activity.[44]
It has been shown that hMG is a safe and effective mode of therapy in increasing testicular size and inducing spermatogenesis in males with hypogonadotrophic hypogonadism.[45] It should be noted though that hCG alone also can induce spermatogenesis (which implies that is has some FSH activity).[46]
As of this writing, there is only one published study on the use of hMG together with hCG anabolic steroid-induced azoospermia (no sperm count) that was persistent 1 year after cessation from steroid use.[47] This case report was a married couple with primary subfertility secondary to azoospermia and male hypogonadotropic hypogonadism. The husband was a bodybuilder who admitted to have used the anabolic steroids testosterone cypionate, methandrostenolone, oxandrolone, testosterone propionate, oxymetholone, nandrolone decanoate, and methenolone enanthate.[47] He was given twice-weekly injections of 10,000 IU of hCG (Profasi; Serono) and daily injections of 75 IU of hMG (Humegon; Organon) for 3 months. Results showed that semen parameters returned to normal after 3 months of treatment and the couple conceived spontaneously 7 months later.[47] It was concluded that anabolic steroid-induced azoospermia that is persistent after cessation of steroid use may be treated successfully with hCG and hMG.[47]
However, there is currently no study available that has compared head-to-head hCG alone, hMG alone, and hCG + hMG together, for restoring testosterone levels and/or fertility in men who have used anabolic steroids. Thus it is not clear if the same response could have been achieved using hCG alone. The speed of recovery of endocrine function in this case study did not seem to be any faster than the previously reported case using hCG alone (the young competitive bodybuilder).[24] The relative merit of hMG is therefore unknown. Also, it should be noted that hMG is very expensive.
A clinical study on men with isolated hypogonadotrophic hypogonadism (not caused by anabolic steroids) demonstrated that hCG alone (1500 IU 3 times per week) is an effective treatment to induce complete spermatogenesis in this patient population, regardless of their initial testicular volume.[46] However, it was noted that a number of these patients may benefit in terms of testicular volume, sperm output, and pregnancy outcome, from the addition of hMG (75 IU subcutaneously 3 times per week).[46]
It should be underscored that results obtained in studies on different clinical populations may differ from those in post-anabolic steroid users, and extrapolations therefore should be done cautiously.
Clomiphene – aka Clomid
Anabolic steroid administration often causes substantial elevations in estradiol (the main estrogen) levels.[48, 49] Estradiol has a much stronger inhibitory effect on the pituitary than testosterone, being 200-fold more effective in suppressing LH secretion.[50-54] DHT (dihydrotestosterone), either from endogenous conversion of testosterone or from DHT administration, does not significantly alter gonadotropin secretion.[51] Estradiol has dual sites of negative feedback, acting at the hypothalamus to decrease GnRH pulse frequency and at the pituitary to decrease responsiveness to GnRH.[50, 52] When looking at the gonadotropins separately, testosterone exerts both direct and indirect feedback on LH secretion, whereas its effects on FSH appear to be mediated largely by aromatization (conversion) to estradiol.[55] When looking at the sites of action, inhibition of LH by testosterone requires aromatization for its pituitary, but not hypothalamic effects, while estradiol negative feedback on LH occurs at the hypothalamic level.[56]
Clomid works by blocking estradiol action in the pituitary.[57] The pituitary thereby sees less estrogen and makes more LH and FSH due to removal of negative feedback inhibition from estrogen.[58-61] Increased LH levels in turn stimulate the Leydig cells in the testis to produce testosterone, while the increased FSH stimulates Sertoli cells in the testis to produce sperma.[59, 60] This is why clomid may be used to treat testosterone deficiency (aka hypogonadism) and infertility in men.[61-67]
At a dose of 100 mg/day for 2 months, clomid has also been shown to successfully reverse testosterone deficiency symptoms, restore testosterone levels, LH surges and the hypothlamic-pituitary-gonadal axis in a 30 year old male patient whose axis was previously shut off due to multiple anabolic steroid abuse.[68]
Clomid can also restore disruption of the HPG-axis induced by excessive exercise such as marathon running.[69] In a case report, reestablishment of HPG-axis functioning with the return of normal testosterone levels and gonadal function was achieved with clomid treatment (50 mg, 2 times per day) over 5 months.
Looking at the clomid dosages used for restoration of HPG-axis function after anabolic steroid use (or due to marathon running) one can concluded that much higher dosages are needed, in the range of 100 mg per day [68, 69], than what is needed to treat testosterone deficiency and infertility, where doses of 25 mg per day seem to be enough.[61-67]
Clomid is comprised of a 38% / 62% mixture of cis and trans isomers, zuclomiphene and enclomiphene, respectively (note: isomers are compounds with the same chemistry formula but a different arrangement of atoms in the molecule and different properties).[70] It is enclomiphene that anatagonizes (inhibits the activity of) estrogen receptors in the hypothalamus and exerts the anti-estrogen.[70] Zuclomiphene actually has estrogenic effects.[70] Therefore, when using clomid as part of post-cycle therapy, the addition of tamoxifen (another anti-estrogen) might be expected to increase the overall antagonism of the estradiol receptor, and thereby the efficacy.[27]
While clomid may be an effective option to treat testosterone deficiency and infertility in men, it is important to note that it does reduce GH (growth hormone) secretion [71], lowers IGF-1 levels[72], and elevates SHBG levels (thereby lowering active free testosterone levels).[72] Clomid is actually so effective in reducing IGF-1 levels that is it being considered a treatment option in acromegaly patients (who are characterized by elevated IGF-1 levels).[73] Therefore, during clomid treatment it is important to monitor the IGF-1 levels and SHBG and free testosterone levels, in addition to total testosterone levels.
Enclomiphene – aka Enclomid
As mentioned above, it is the enclomiphene part of clomid that induces hypothalamic GnRH release, thus increasing serum testosterone levels. Treatment with zuclomiphene alone actually can reduce testosterone to near-castrate levels.[74] Therefore, pure enclomiphene preparations have been developed. In the US, a pure enclomiphene preparation called Androxal is undergoing phase II/III clinical trials. So far, the study results are promising, showing that encolomiphene increases levels of both LH, FSH, testosterone and sperm counts.[75, 76] This is in stark contrast to treatment with testosterone, which profoundly reduces LH and FSH levels, as well as sperm parameters. For more info, see my previous article “TRT and Fertility – how to get the best of both worlds – part 1”. Thus, if enclomiphene gets FDA approval, its off-label use for post cycle therapy will likely become very effective and popular.
GnRH (Gonadotrophin-Releasing Hormone)
Natural LH and FSH secretion is tightly regulated by hypothalamic GnRH secretion.[77] GnRH is normally secreted in brief bursts from hypothalamic neurons into the pituitary portal (blood) system and controls the physiological pattern of blood LH levels, which are highly pulsatile with peaks at 60- to 90-min intervals.[78, 79]
Administration of exogenous GnRH in any non-pulsatile fashion rapidly desensitizes pituitary and suppresses the secretion of LH and FSH, which only recovers when intermittent GnRH administration is restored.[78, 79] Consequently, replicating physiological pulsatility by intermittent delivery of brief bursts of GnRH is critical to maintain physiological circulating levels of LH, FSH and testosterone.
One study tested the effect of a single hCG dose (50 units/kg im) in six anabolic-using power athletes. Results showed an attenuated acute testosterone rise (similar to that seen in the pre-pubertal state), and the scientists suggested that FSH/LH priming may be necessary for an adequate response.[38] Exogenous GnRH administration induces pituitary and gonadal priming, which subsequently enable men to sustain normal pituitary and gonadal function in response to their own weakened GnRH secretion.[80]
Initial support for the efficacy of LH/FSH priming comes from a case-study of a 34 year old bodybuilder who had been on anabolic steroids since age 21.[81] At baseline his testosterone level was 170 ng/dL. 10 days after a triptorelin challenge (aka triptorelin test), which is a single dose (100 mg) of the GnRH agonist called triptorelin, he reported a great amelioration of energy, and his testosterone levels increased to 700 ng/dL. One month later, his testosterone level was within the normal range, and he reported a return to normal libido and energy.[81]
A recent notable study from the Center for Andrology and Sexual Medicine at The Karolinska University Hospital further shows that the GnRH test, as well as hCG test, may be valuable clinical tools to evaluate the HPG-axis in men with previous history of anabolic steroid use, and provide valuable information in clinical management of these men.[82] This study shows that using both GnRH and hCG tests in men with anabolic steroid induced hypogonadism allows for discrimination of primary hypothalamic/pituitary failures versus testicular failure (Leydig cell insufficiency). Specifically, those who respond to a GnRH test may be the ones who will benefit the most from elimination negative feedback regulators, such as estradiol, by means of anti-estrogens or aromatase inhibitors.
Post Cycle Therapy – treatment examples
There is a relative paucity of studies dealing specifically with anabolic steroid induced hypogonadism, and how to best restore normal endocrine function and spermatogenesis.
What follows is a report of two poster child cases of anabolic steroid using bodybuilders who were successfully treated with combined therapies using some of the medications outlined above. All post-therapy blood tests were taken 15 days after the last hCG injection.
Case 1: [83]
6’0″ 206 lbs. 33 year old Caucasian male with a 10+ year history of steroid self-administration for bodybuilding and powerlifting. By his own admission he was a “heavy” user, taking from 500 mg/week to 2+ grams/week.
Pre-treatment values: LH < 1.0 IU/L, testosterone 191 ng/dL.
One course of therapy (32 days) was given:
2,500 IU of hCG every 4 days (8 injections total), 50 mg clomiphene twice daily and 10 mg tamoxifen once daily.
Despite massive drug use patient was an exceptionally good responder.
Post-treatment values: LH 5.2 IU/L, testosterone 1072 ng/dL.
Case 2: [83]
5’10″ 184 lbs 36 year old Caucasian male with a 2 year history of continuous nandrolone use, 200-400 mg/week.
Pre-values: LH < 1.0 IU/L, testosterone 45 ng/dL.
Treatment 1 (32 days):
2,500 IU hCG every 4 d (8 total), clomiphene (50 mg twice daily) and arimidex (1 mg once daily.).
Post-values: LH < 1.0 IU/L, testosterone 38 ng/dL. Treatment 2 (60 days): 5,000 IU hCG every 4 days (4 injections total) followed by 2,500 IU hCG every 4 d (4 injections total), clomiphene (50 mg twice daily) and tamoxifen (10 mg once daily). Post-values: LH > 1.4 IU/L, testosterone 63 ng/dL.
Treatment 3 (32 days):
5,000 IU hCG every other day (6 injections total) followed by 2,500 IU hCG every other day (6 injections total) given simultaneously with menotropin 150 IU every other day (6 injections total), clomiphene (50 mg twice daily) and tamoxifen (10 mg once daily).
Post-values: LH 9.8 IU/L, testosterone 507 ng/dL.
Comments on the case reports:
As was shown in these exemplary cases, restoration of the HPG-axis, even after heavy use of anabolic steroids, is possible with combined therapies and careful monitoring. However, FSH, testicular volumes and sperma parameters were not reported in these cases. Further research is needed in this area.
Other essential elements of PCT – blood lipids, adrenals and the liver
Use of anabolic steroids not only affects the HPG-axis. It also harmfully impacts the blood lipid profile (i.e. the distribution of cholesterol, blood fats and lipoproteins) and commonly causes dyslipidemia. It suppresses adrenal function. The anabolic steroid induced adrenal suppression is relatively unknown, to both users as well as doctors.
The effects of anabolic steroid on liver function are widely touted. However, this is controversial, as most doctors rely solely on liver enzyme elevations to diagnose liver dysfunction. In athletes and hard training fitness enthusiasts, liver enzymes are frequently elevated even in people who have not taken anabolic steroids. Therefore, other labs need to be included in order to make a correct diagnosis of liver dysfunction in anabolic steroid users.
Post cycle therapy needs to address these health issues as well; it is critical to go to a doctor who knows not only how to restore the HPG-axis, but also how to treat an atherogenic blood lipid profile, suppressed adrenals, and how to correctly evaluate liver function. I will cover all these issues in an upcoming articles…
Summary
The studies and case reports outlined in this article clearly show that there is no “one-size-fits all” post-cycle therapy. Individual characteristics, types and dosages of anabolic steroids used, and duration of use are important factors that will impact the design of an effective post-cycle therapy. Because of this it is important to go to a doctor who is well versed in andrology and endocrine regulation, as well as the side effects of anabolic steroids.
The most commonly used medications for post-cycle therapy are hCG, clomid, tamoxifen and arimidex. In general, hCG is used to treat testicular atrophy while clomid is used to restart the HPG-axis. On the treatment horizon is enclomiphene, which can be seen as a more effective version of clomid. Also, a new potential strategy is LH/FSH priming by a GnRH challenge (the triptorelin test).
Most physicians are uncomfortable addressing anabolic steroid use and are hesitant to broach the topic with patients.[26] To effectively manage these patients, it is imperative that physicians know the varying side effect profiles of different anabolic steroids and understands user’s cycles, stacks and motives. Dr. Pierce at Ageless Forever – www.agelessforever.net – is one of the few who does. Being a former athlete himself, Dr. Pierce understands the mentality of anabolic steroid users and knows the underground lingo. In addition, Dr. Pierce stays on top of medical research in order to provide the best possible individualized care for his patients, many of whom are anabolic steroid users.
About the Author:
————————————–

Monica Mollica has a Bachelor’s and Master’s degree in Nutrition from the University of Stockholm, Sweden, and is an ISSA Certified Personal Trainer. She works a dietary consultant, health journalist and writer for www.BrinkZone.com, and is also a web designer and videographer.
Monica has admired and been fascinated by muscular and sculptured strong athletic bodies since childhood, and discovered bodybuilding as an young teenager. Realizing the importance of nutrition for maximal results in the gym, she went for a BSc and MSc with a major in Nutrition at the University.
During her years at the University she was a regular contributor to the Swedish bodybuilding magazine BODY, and she has published the book (in Swedish) “Functional Foods for Health and Energy Balance”, and authored several book chapters in Swedish publications.
It was her insatiable thirst for knowledge and scientific research in the area of bodybuilding and health that brought her to the US. She has completed one semester at the PhD-program “Exercise, Nutrition and Preventive Health” at Baylor University Texas, at the department of Health Human Performance and Recreation, and worked as an ISSA certified personal trainer. Today, Monica is sharing her solid experience by doing dietary consultations and writing about topics related to health, fitness, bodybuilding, anti-aging and longevity. www.trainergize.com
References:
1. Pope, H.G., Jr., et al., The lifetime prevalence of anabolic-androgenic steroid use and dependence in Americans: current best estimates. Am J Addict, 2014. 23(4): p. 371-7.
2. Hartgens, F. and H. Kuipers, Effects of androgenic-anabolic steroids in athletes. Sports Med, 2004. 34(8): p. 513-54.
3. Casavant, M.J., et al., Consequences of use of anabolic androgenic steroids. Pediatr Clin North Am, 2007. 54(4): p. 677-90, x.
4. Fronczak, C.M., E.D. Kim, and A.B. Barqawi, The insults of illicit drug use on male fertility. J Androl, 2012. 33(4): p. 515-28.
5. Garevik, N., et al., Long term perturbation of endocrine parameters and cholesterol metabolism after discontinued abuse of anabolic androgenic steroids. J Steroid Biochem Mol Biol, 2011. 127(3-5): p. 295-300.
6. Jarow, J.P. and L.I. Lipshultz, Anabolic steroid-induced hypogonadotropic hypogonadism. Am J Sports Med, 1990. 18(4): p. 429-31.
7. de Souza, G.L. and J. Hallak, Anabolic steroids and male infertility: a comprehensive review. BJU Int, 2011. 108(11): p. 1860-5.
8. Kanayama, G., et al., Prolonged hypogonadism in males following withdrawal from anabolic-androgenic steroids: an under-recognized problem. Addiction, 2015.
9. Youssef, M.Y., A. Alqallaf, and N. Abdella, Anabolic androgenic steroid-induced cardiomyopathy, stroke and peripheral vascular disease. BMJ Case Rep, 2011. 2011.
10. Angell, P., et al., Anabolic steroids and cardiovascular risk. Sports Med, 2012. 42(2): p. 119-34.
11. Angell, P.J., et al., Anabolic steroid use and longitudinal, radial, and circumferential cardiac motion. Med Sci Sports Exerc, 2012. 44(4): p. 583-90.
12. Angell, P.J., et al., Performance enhancing drug abuse and cardiovascular risk in athletes: implications for the clinician. Br J Sports Med, 2012. 46 Suppl 1: p. i78-84.
13. Angell, P.J., et al., Ventricular structure, function, and focal fibrosis in anabolic steroid users: a CMR study. Eur J Appl Physiol, 2014. 114(5): p. 921-8.
14. Baggish, A.L., et al., Long-term anabolic-androgenic steroid use is associated with left ventricular dysfunction. Circ Heart Fail, 2010. 3(4): p. 472-6.
15. Deligiannis, A.P. and E.I. Kouidi, Cardiovascular adverse effects of doping in sports. Hellenic J Cardiol, 2012. 53(6): p. 447-57.
16. Pope, H.G., Jr., et al., Adverse health consequences of performance-enhancing drugs: an Endocrine Society scientific statement. Endocr Rev, 2014. 35(3): p. 341-75.
17. Kersey, R.D., et al., National Athletic Trainers’ Association position statement: anabolic-androgenic steroids. J Athl Train, 2012. 47(5): p. 567-88.
18. Hoffman, J.R., et al., Position stand on androgen and human growth hormone use. J Strength Cond Res, 2009. 23(5 Suppl): p. S1-S59.
19. Achar, S., A. Rostamian, and S.M. Narayan, Cardiac and metabolic effects of anabolic-androgenic steroid abuse on lipids, blood pressure, left ventricular dimensions, and rhythm. Am J Cardiol, 2010. 106(6): p. 893-901.
20. Basaria, S., Androgen abuse in athletes: detection and consequences. J Clin Endocrinol Metab, 2010. 95(4): p. 1533-43.
21. Matsumoto, A.M. and W.J. Bremner, Modulation of pulsatile gonadotropin secretion by testosterone in man. J Clin Endocrinol Metab, 1984. 58(4): p. 609-14.
22. Palacios, A., et al., Effect of testosterone enanthate on testis size. J Urol, 1981. 126(1): p. 46-8.
23. MacIndoe, J.H., et al., Testosterone suppression of the HPT axis. J Investig Med, 1997. 45(8): p. 441-7.
24. Gill, G.V., Anabolic steroid induced hypogonadism treated with human chorionic gonadotropin. Postgrad Med J, 1998. 74(867): p. 45-6.
25. Coward, R.M., et al., Anabolic steroid induced hypogonadism in young men. J Urol, 2013. 190(6): p. 2200-5.
26. Rahnema, C.D., et al., Anabolic steroid-induced hypogonadism: diagnosis and treatment. Fertil Steril, 2014. 101(5): p. 1271-9.
27. Tan, R.S. and M.C. Scally, Anabolic steroid-induced hypogonadism–towards a unified hypothesis of anabolic steroid action. Med Hypotheses, 2009. 72(6): p. 723-8.
28. Medras, M., et al., Clomiphene Stimulation Test in Men Abusing Anabolic-Androgenic Steroids for Long Time. . J Steroids Hormon Sci, 2014. 4.
29. Brower, K.J., et al., Symptoms and correlates of anabolic-androgenic steroid dependence. Br J Addict, 1991. 86(6): p. 759-68.
30. Ip, E.J., et al., Psychological and physical impact of anabolic-androgenic steroid dependence. Pharmacotherapy, 2012. 32(10): p. 910-9.
31. Hildebrandt, T., et al., Exercise reinforcement, stress, and beta-endorphins: an initial examination of exercise in anabolic-androgenic steroid dependence. Drug Alcohol Depend, 2014. 139: p. 86-92.
32. Kanayama, G., et al., Treatment of anabolic-androgenic steroid dependence: Emerging evidence and its implications. Drug Alcohol Depend, 2010. 109(1-3): p. 6-13.
33. Kanayama, G., et al., Anabolic-androgenic steroid dependence: an emerging disorder. Addiction, 2009. 104(12): p. 1966-78.
34. Kashkin, K.B. and H.D. Kleber, Hooked on hormones? An anabolic steroid addiction hypothesis. JAMA, 1989. 262(22): p. 3166-70.
35. Ahmed, M.A., Amelioration of nandrolone decanoate-induced testicular and sperm toxicity in rats by taurine: effects on steroidogenesis, redox and inflammatory cascades, and intrinsic apoptotic pathway. Toxicol Appl Pharmacol, 2015. 282(3): p. 285-96.
36. van Breda, E., et al., Androgenic anabolic steroid use and severe hypothalamic-pituitary dysfunction: a case study. Int J Sports Med, 2003. 24(3): p. 195-6.
37. Moretti, E., et al., Structural sperm and aneuploidies studies in a case of spermatogenesis recovery after the use of androgenic anabolic steroids. J Assist Reprod Genet, 2007. 24(5): p. 195-8.
38. Martikainen, H., et al., Testicular responsiveness to human chorionic gonadotrophin during transient hypogonadotrophic hypogonadism induced by androgenic/anabolic steroids in power athletes. J Steroid Biochem, 1986. 25(1): p. 109-12.
39. Matsumoto, A.M., et al., Human chorionic gonadotropin and testicular function: stimulation of testosterone, testosterone precursors, and sperm production despite high estradiol levels. J Clin Endocrinol Metab, 1983. 56(4): p. 720-8.
40. Coviello, A.D., et al., Low-dose human chorionic gonadotropin maintains intratesticular testosterone in normal men with testosterone-induced gonadotropin suppression. J Clin Endocrinol Metab, 2005. 90(5): p. 2595-602.
41. Hsieh, T.C., et al., Concomitant intramuscular human chorionic gonadotropin preserves spermatogenesis in men undergoing testosterone replacement therapy. J Urol, 2013. 189(2): p. 647-50.
42. Karila, T., O. Hovatta, and T. Seppala, Concomitant abuse of anabolic androgenic steroids and human chorionic gonadotrophin impairs spermatogenesis in power athletes. Int J Sports Med, 2004. 25(4): p. 257-63.
43. Schiff, J.D., M.L. Ramirez, and N. Bar-Chama, Medical and surgical management male infertility. Endocrinol Metab Clin North Am, 2007. 36(2): p. 313-31.
44. Practice Committee of American Society for Reproductive Medicine, B.A., Gonadotropin preparations: past, present, and future perspectives. Fertil Steril, 2008. 90(5 Suppl): p. S13-20.
45. Jones, T.H. and J.F. Darne, Self-administered subcutaneous human menopausal gonadotrophin for the stimulation of testicular growth and the initiation of spermatogenesis in hypogonadotrophic hypogonadism. Clin Endocrinol (Oxf), 1993. 38(2): p. 203-8.
46. Vicari, E., et al., Therapy with human chorionic gonadotrophin alone induces spermatogenesis in men with isolated hypogonadotrophic hypogonadism–long-term follow-up. Int J Androl, 1992. 15(4): p. 320-9.
47. Menon, D.K., Successful treatment of anabolic steroid-induced azoospermia with human chorionic gonadotropin and human menopausal gonadotropin. Fertil Steril, 2003. 79 Suppl 3: p. 1659-61.
48. Urhausen, A., A. Torsten, and K. Wilfried, Reversibility of the effects on blood cells, lipids, liver function and hormones in former anabolic-androgenic steroid abusers. J Steroid Biochem Mol Biol, 2003. 84(2-3): p. 369-75.
49. Lakshman, K.M., et al., The effects of injected testosterone dose and age on the conversion of testosterone to estradiol and dihydrotestosterone in young and older men. J Clin Endocrinol Metab, 2010. 95(8): p. 3955-64.
50. Hayes, F.J., et al., Aromatase inhibition in the human male reveals a hypothalamic site of estrogen feedback. J Clin Endocrinol Metab, 2000. 85(9): p. 3027-35.
51. Bagatell, C.J., K.D. Dahl, and W.J. Bremner, The direct pituitary effect of testosterone to inhibit gonadotropin secretion in men is partially mediated by aromatization to estradiol. J Androl, 1994. 15(1): p. 15-21.
52. Finkelstein, J.S., et al., Sex steroid control of gonadotropin secretion in the human male. II. Effects of estradiol administration in normal and gonadotropin-releasing hormone-deficient men. J Clin Endocrinol Metab, 1991. 73(3): p. 621-8.
53. Veldhuis, J.D. and M.L. Dufau, Estradiol modulates the pulsatile secretion of biologically active luteinizing hormone in man. J Clin Invest, 1987. 80(3): p. 631-8.
54. Schnorr, J.A., M.J. Bray, and J.D. Veldhuis, Aromatization mediates testosterone’s short-term feedback restraint of 24-hour endogenously driven and acute exogenous gonadotropin-releasing hormone-stimulated luteinizing hormone and follicle-stimulating hormone secretion in young men. J Clin Endocrinol Metab, 2001. 86(6): p. 2600-6.
55. Hayes, F.J., et al., Differential regulation of gonadotropin secretion by testosterone in the human male: absence of a negative feedback effect of testosterone on follicle-stimulating hormone secretion. J Clin Endocrinol Metab, 2001. 86(1): p. 53-8.
56. Pitteloud, N., et al., Inhibition of luteinizing hormone secretion by testosterone in men requires aromatization for its pituitary but not its hypothalamic effects: evidence from the tandem study of normal and gonadotropin-releasing hormone-deficient men. J Clin Endocrinol Metab, 2008. 93(3): p. 784-91.
57. Kim, E.D., et al., The treatment of hypogonadism in men of reproductive age. Fertil Steril, 2013. 99(3): p. 718-24.
58. Dickey, R.P., et al., Observations on the mechanism of action of clomiphene (MRL-41). Fertil Steril, 1965. 16(4): p. 485-94.
59. Patankar, S.S., et al., Effect of clomiphene citrate on sperm density in male partners of infertile couples. Indian J Physiol Pharmacol, 2007. 51(2): p. 195-8.
60. Schellen, T.M., Clomiphene treatment in male infertility. Int J Fertil, 1982. 27(3): p. 136-45.
61. Guay, A.T., S. Bansal, and G.J. Heatley, Effect of raising endogenous testosterone levels in impotent men with secondary hypogonadism: double blind placebo-controlled trial with clomiphene citrate. J Clin Endocrinol Metab, 1995. 80(12): p. 3546-52.
62. Guay, A.T., et al., Clomiphene increases free testosterone levels in men with both secondary hypogonadism and erectile dysfunction: who does and does not benefit? Int J Impot Res, 2003. 15(3): p. 156-65.
63. Shabsigh, A., et al., Clomiphene citrate effects on testosterone/estrogen ratio in male hypogonadism. J Sex Med, 2005. 2(5): p. 716-21.
64. Tenover, J.S. and W.J. Bremner, The effects of normal aging on the response of the pituitary-gonadal axis to chronic clomiphene administration in men. J Androl, 1991. 12(4): p. 258-63.
65. Moskovic, D.J., et al., Clomiphene citrate is safe and effective for long-term management of hypogonadism. BJU Int, 2012. 110(10): p. 1524-8.
66. Katz, D.J., et al., Outcomes of clomiphene citrate treatment in young hypogonadal men. BJU Int, 2012. 110(4): p. 573-8.
67. Da Ros, C.T. and M.A. Averbeck, Twenty-five milligrams of clomiphene citrate presents positive effect on treatment of male testosterone deficiency – a prospective study. Int Braz J Urol, 2012. 38(4): p. 512-8.
68. Tan, R.S. and D. Vasudevan, Use of clomiphene citrate to reverse premature andropause secondary to steroid abuse. Fertil Steril, 2003. 79(1): p. 203-5.
69. Burge, M.R., et al., Idiopathic hypogonadotropic hypogonadism in a male runner is reversed by clomiphene citrate. Fertil Steril, 1997. 67(4): p. 783-5.
70. Glasier, A.F., et al., A comparison of the effects on follicular development between clomiphene citrate, its two separate isomers and spontaneous cycles. Hum Reprod, 1989. 4(3): p. 252-6.
71. Perlow, M., et al., Reduction of growth hormone secretion following clomiphene administration. Metabolism, 1973. 22(10): p. 1269-75.
72. Butzow, T.L., L.M. Kettel, and S.S. Yen, Clomiphene citrate reduces serum insulin-like growth factor I and increases sex hormone-binding globulin levels in women with polycystic ovary syndrome. Fertil Steril, 1995. 63(6): p. 1200-3.
73. Duarte, F.H., R.S. Jallad, and M.D. Bronstein, Clomiphene citrate for treatment of acromegaly not controlled by conventional therapies. J Clin Endocrinol Metab, 2015: p. jc20143913.
74. Hill, S., V. Arutchelvam, and R. Quinton, Enclomiphene, an estrogen receptor antagonist for the treatment of testosterone deficiency in men. IDrugs, 2009. 12(2): p. 109-19.
75. Kaminetsky, J., et al., Oral enclomiphene citrate stimulates the endogenous production of testosterone and sperm counts in men with low testosterone: comparison with testosterone gel. J Sex Med, 2013. 10(6): p. 1628-35.
76. Wiehle, R., et al., Testosterone Restoration by Enclomiphene Citrate in Men with Secondary Hypogonadism: Pharmacodynamics and Pharmacokinetics. BJU Int, 2013.
77. Keenan, D.M., et al., An ensemble model of the male gonadal axis: illustrative application in aging men. Endocrinology, 2006. 147(6): p. 2817-28.
78. Belchetz, P.E., et al., Hypophysial responses to continuous and intermittent delivery of hypopthalamic gonadotropin-releasing hormone. Science, 1978. 202(4368): p. 631-3.
79. Nakai, Y., et al., On the sites of the negative and positive feedback actions of estradiol in the control of gonadotropin secretion in the rhesus monkey. Endocrinology, 1978. 102(4): p. 1008-14.
80. Finkelstein, J.S., et al., Pulsatile gonadotropin secretion after discontinuation of long term gonadotropin-releasing hormone (GnRH) administration in a subset of GnRH-deficient men. J Clin Endocrinol Metab, 1989. 69(2): p. 377-85.
81. Pirola, I., et al., Anabolic steroids purchased on the Internet as a cause of prolonged hypogonadotropic hypogonadism. Fertil Steril, 2010. 94(6): p. 2331 e1-3.
82. Flanagan, J.N. and M. Lehtihet, The Response to Gonadotropin-Releasing Hormone and hCG in Men with Prior Chronic Androgen Steroid Abuse and Clinical Hypogonadism. Horm Metab Res, 2015.
83. Street, C. and M.C. Scally, Pharmaceutical intervention of anabolic steroid induced hypogonadism – our success at restoration of the HPG axis. . Med Sci Sports Exerc, 2000. 32(Suppl. 5).

