

 Testosterone replacement therapy is not without side effects, although most are manageable. I’ve been taking testosterone replacement for 16 years and for the most part have had few side effects thanks to careful monitoring. It’s critical that you are monitored for side effects in addition to your testosterone level. Some men may experience one or more side effects that sometimes go unnoticed until it is too late. In part it is the underground, unmonitored use of testosterone that creates so much bad publicity for a very helpful product. The first step in the proper monitoring of replacement therapy is providing your doctor with a thorough medical history. Appendix A shows a simple and comprehensive medical history form (courtesy of Dr John Crisler, allthingsmale.com). Patients who would like to be proactive can fill out this form and give a copy to their doctor. It is expected that every doctor have a similar form, although most do not ask questions pertinent to sexual function or on the use of androgens. Let your doctor know about all the medications you take so that medication-induced sexual dysfunction can be ruled out before starting testosterone.I also strongly believe that if a patient goes to the doctor to obtain a Viagra, Cialis or Levitra prescription, the doctor should check the patient’s testosterone blood levels to ensure that it is not the root of the problem. Hypogonadal men may not respond as well to these drugs if their testosterone is not normalized first. Studies combining testosterone and oral sexual enhancement drugs have shown a synergistic effect on sexual benefits. The following suggested guidelines for monitoring testosterone replacement is recommended by several physician groups and practices:
Testosterone replacement therapy is not without side effects, although most are manageable. I’ve been taking testosterone replacement for 16 years and for the most part have had few side effects thanks to careful monitoring. It’s critical that you are monitored for side effects in addition to your testosterone level. Some men may experience one or more side effects that sometimes go unnoticed until it is too late. In part it is the underground, unmonitored use of testosterone that creates so much bad publicity for a very helpful product. The first step in the proper monitoring of replacement therapy is providing your doctor with a thorough medical history. Appendix A shows a simple and comprehensive medical history form (courtesy of Dr John Crisler, allthingsmale.com). Patients who would like to be proactive can fill out this form and give a copy to their doctor. It is expected that every doctor have a similar form, although most do not ask questions pertinent to sexual function or on the use of androgens. Let your doctor know about all the medications you take so that medication-induced sexual dysfunction can be ruled out before starting testosterone.I also strongly believe that if a patient goes to the doctor to obtain a Viagra, Cialis or Levitra prescription, the doctor should check the patient’s testosterone blood levels to ensure that it is not the root of the problem. Hypogonadal men may not respond as well to these drugs if their testosterone is not normalized first. Studies combining testosterone and oral sexual enhancement drugs have shown a synergistic effect on sexual benefits. The following suggested guidelines for monitoring testosterone replacement is recommended by several physician groups and practices:
You should be evaluated after the first month of therapy to measure your testosterone blood levels. If your doctor doesn’t ask, let him know about your quality of life. Make sure your doctor is aware of your energy level, mood, and sexual function, as well as any potential side effects (tender breasts, urinary flow decrease, moodiness, and acne).
When using testosterone, your doctor will want to measure total blood testosterone levels right before the next corresponding injection after the first month (it takes a while for the blood levels to stabilize). If testosterone is >700 ng/dl (24.5 nmol/liter) or <350 ng/dl (12.3 nmol/liter), your doctor will adjust the amount or the frequency of your dose. I mentioned this earlier in the book but it bears repeating here: Some men need to have levels above 500 ng/dl to experience any of the expected sexual function benefits from testosterone. It is important to be honest about when your doctor asks you about your sexual performance.
Your doctor will check your hematocrit before starting testosterone, after 3 months and then every year after that. If your hematocrit is above 54%, you may need a therapeutic phlebotomy (read the section "Checking for Increased Blood Thickness (Polycythemia)" for more details.
Be ready to have a digital rectal examination done and a prostatic specific antigen (PSA) blood test drawn prior to starting testosterone, and after 3 months. Once every 6 months after that may not be unreasonable, especially in older men. A PSA over 4 ng/ml can be reason for concern and referral to an urologist. Testosterone replacement needs to be stopped if increases in PSA above normal are observed. Note: at the start of testosterone replacement in older men, when testosterone blood levels are rapidly rising, PSA may also increase. This is especially true when testosterone gels are employed, because they elevate DHT more relative to other options. Once testosterone levels have stabilized PSA drops back down to roughly baseline. It is important to allow "steady state" for testosterone fluctuations to stabilize before measuring PSA; a month or so should be sufficient.
If you start experiencing breast tenderness, pain or growth, ask your doctor to measure your estradiol blood level using the sensitive assay (not the regular test used for women). Normal range for estradiol in men is 14–54 pg/ml (50–200 pmol/liter). Men who have high estradiol can be prescribed estrogen receptor inhibitors (more details in "Avoiding enlarged breasts (gynecomastia)"
LOOK INSIDE TH EBOOK (FIRST 20 PAGES) http://issuu.com/nelsonvergel/docs/aatestosteronefirst20pages
What Is Testosterone and How Does It Work?
Testosterone is the hormone responsible for normal growth and development and maintenance of male sex characteristics. It also affects lean body mass, mood and sexual function in both males and females. It is the primary androgenic (responsible for masculine characteristics) and anabolic (muscle building) hormone.Testosterone is produced by the testicles in males and by the ovaries in females, with small amounts also produced by the adrenal glands in both genders. Its production and secretion are regulated by other hormones in a hormonal cascade.
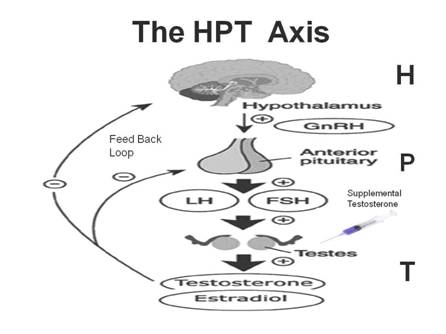
As shown in Figure 1, the hormonal and reproductive function of the testicles (gonads) is regulated through interactions among the hypothalamus, the pituitary gland, and the gonads (commonly known as the hypothalamic-pituitary-gonadal axis [HPGA]). The three glands communicate through a cascade of hormones and a self-regulating feedback loop that controls the generation of each hormone. Release of gonadotropin-releasing hormone (GnRH) from the hypothalamus regulates secretion of other hormones (gonadotropins) that influence the testicles by way of the pituitary. GnRH controls the secretion of luteinizing hormone (LH) and follicle-stimulating hormone (FSH) by the anterior pituitary. Luteinizing hormone regulates the production and secretion of testosterone through the Leydig cells of the testes, while FSH stimulates the production of sperm.
Figure 1. Hormonal cascade that regulates testosterone production in malesWhen someone is found to have low testosterone blood levels this is known as “hypogonadism” There are several types of hypogonadism:
- Primary hypogonadism is a hypergonadotropic condition (higher than normal levels of LH and FSH). This occurs when the testicles fail to produce sufficient levels of testosterone to suppress production of LH and FSH. As a result, LH and FSH levels are elevated while testosterone levels are decreased. The pituitary glands tried to increase testosterone at no avail even after increasing LH and FSH.
- Secondary hypogonadism results from hypothalamic or pituitary dysfunction. It is characterized by disruption of central components of the HPGA resulting in decreased levels of GnRH, LH, or FSH. In this type of hypogonadism, low levels of LH do not allow for the proper stimulation of the production of testosterone by the testes.
- Mixed hypogonadism results from a combination of primary and secondary causes. The most common cause of mixed hypogonadism is late-onset hypogonadism, which occurs with aging. This is associated with osteoporosis, decreased lean body mass, reduced cognition, fatigue and impairment of libido and erectile function. Other causes of mixed hypogonadism include alcoholism, diseases (such as uremia, liver failure, AIDS, and sickle cell disease), street drugs/alcohol, and medications like corticosteroid steroids used for inflammatory conditions. It should be noted that high levels of cortisol (hypercortisolism), resulting from either the use of anti-inflammatory steroids or physical causes, could lead to hypogonadism.
Figure 2: Testosterone MetabolitesAs shown in Figure 2, testosterone in the body can convert into other hormones and metabolites. The process in which testosterone is converted into estrogen (a female hormone) by the aromatase enzyme is known as “aromatization”. Males with high body fat, aging males, males taking certain medications, Males with sex chromosome genetic conditions such as Klinefelters Syndrome or males with a genetic disposition to having higher than normal amounts of aromatase may experience higher conversion of testosterone into estrogen. Estrogen blood levels are usually measured by detecting estradiol, the main estrogen in humans.
Estrogen is a very important hormone for men at the right concentration. It plays an important role in bone, hair, skin, and brain health as well as other functions in men. Large amounts of estrogen can cause mood swings, enlarged breasts (gynecomastia), fat gain, and water retention.
Another metabolite of testosterone is dihydrotestosterone (DHT). DHT has a positive effect on sexual desire but increases the production of excess skin oil, which can cause acne, hair loss, and prostatic inflammation. So, it is important to monitor and determine the proper dosage of testosterone so that estradiol and DHT are kept within reference ranges needed for healthy body function as well as to prevent unwanted side effects of TRT.
As shown in Figure 3, about 2 percent of the testosterone in the body is active. This “free testosterone” is not attached to binding proteins that would prevent it from interacting with its receptor.
About 40 percent of the body’s testosterone is attached to albumin. This is a protein that can release the hormone as the need for it arises in the body. Free testosterone and testosterone attached to albumin are referred to as “bioavailable testosterone”.
In a healthy young male, about 60 percent of his testosterone is attached to sex hormone binding globulin (SHBG). Hormones bound to SHBG can’t be used by the body and lose their anabolic effect. As males grow older or if illness is present, SHBG sweeps up more and more testosterone, lowering free testosterone and its benefits.
Total testosterone is the sum of bioavailable testosterone and testosterone bound to SHBG. Measuring just the total testosterone in the blood may not provide the whole picture and let you know how much “active” or usable testosterone you have.
Figure 3. Testosterone fractions in the blood
The normal levels of combined bound and free testosterones in male bodies can range anywhere from 300 to 1,100 ng/dL (nanograms per deciliter). Levels will vary with age and individual factors. It is useful to also measure the level of free testosterone as this may be more indicative of how hormone therapy is progressing. Levels of free testosterone can range between 0.3 and 5 percent of the total testosterone count, with about 2 percent considered an optimal level.
Higher than normal testosterone (i.e., above 1,100 ng/dL of total testosterone) can cause hair loss, acne, mood swings, mania in those with bipolar disorder, water retention, breast enlargement in men, increased aggression and hypersexual behavior, potential prostatic inflammation in older men, increases in the bad cholesterol (low density lipoprotein [LDL]), and decreases in the good cholesterol (high density lipoprotein [HDL]). Like everything in life, balance is key. Too much of a good thing can be detrimental.
Proper monitoring by an experienced physician is extremely important to ensure optimal levels of testosterone, to maximize benefits and to minimize side effects.
Figure 4 Target organs for beneficial and negative effects of testosterone (Courtesy of Dr. Donald Abrams)
What Are the Symptoms of Low Testosterone (Deficiency)?
As mentioned previously, hypogonadism is the medical term for the condition in males that is caused when the body is not producing sufficient amounts of testosterone. What most people don’t realize is that in addition to sexual desire, testosterone also affects lean body mass, strength, bone density, mental focus, mood, fat loss, and other important factors in both males and females (Figure 4).Common complaints for men with hypogonadism include: lower sexual desire (libido), erectile dysfunction (softer erections or lack of erections), depression, low energy and appetite, changes in body composition (lower lean body mass and higher abdominal fat), lower strength, reductions in body and facial hair, less mental focus and decreased height and osteoporosis (decrease in bone density).
As Table 1 shows, normalizing testosterone in people who have lower than normal levels has dramatic benefits, among which are increased sexual desire, lean body mass, bone density, strength, mood, motivation, mental focus, and stamina. However, these benefits can be erased if proper monitoring, dose adjustment, and appropriate choice of testosterone replacement option are not accomplished.
Table 1. Benefits of Normalizing Testosterone
- Restored sexual desire
- Improved erectile function
- Improved mood/ sense of wellbeing
- Increased lean body mass, strength and stamina
- Improved bone density
- Decreased fat mass
Determining If You Have Testosterone Deficiency
In addition to blood tests and physical examination, a brief screening instrument has also been developed by researchers at St. Louis University to aid in the diagnosis of hypogonadism. Known as the Androgen Deficiency in the Aging Male (ADAM) questionnaire:1. Do you have a decrease in sex drive?
2. Do you lack energy?
3. Have you experienced a decrease in strength and/or endurance?
4. Do you feel shorter? Have you lost height? (Lower bone density can decrease height.)
5. Have you noticed a decreased enjoyment of life?
6. Are you sad and/or grumpy?
7. Are your erections less strong or gone?
8. Has it been more difficult to maintain your erection throughout sexual intercourse?
9. Are you falling asleep after dinner?
10. Has your work performance deteriorated recently?Other questions that are usually not asked by doctors, but which I’ve found to be important are the following:
- Are you relating well with people around you?
- Are you being loving to your lover or life partner?
- Are you able to pay attention when someone talks to you?
In my life low testosterone caused problems that went far beyond sex and my body. It affected the way that I related to people and my ability to handle stress at work and in life.
Note that several of the above-mentioned problems can be caused by many other issues unrelated to low testosterone. Depression, anxiety, stress, medications and/or sleep disorders can cause nine of those 10 symptoms (decrease in height would be the only item unrelated to anything but bone loss or back surgery). This questionnaire is not a perfect predictor of low testosterone and should not replace tests for testosterone blood levels.
The benefit of this questionnaire is that it may encourage some men to seek medical advice. Then they can get their testosterone checked and have a physical examination to help determine whether they are indeed hypogonadal.
Causes of Testosterone Deficiency
As discussed before, hypogonadism is caused when the testicles fail to produce normal levels of testosterone. In one type of hypogonadism, testosterone levels are low, while LH and FSH are elevated. In another, there is not enough secretion of LH and FSH needed to tell the testicles to produce needed testosterone.Some commonly used medications such as Megace (an appetite stimulant), Nizoral (an anti-fungal agent), Prednisone (an anti-inflammatory corticosteroid) and Tagamet (an antacid) can also lower testosterone production. Illness and aging can cause a decrease in testosterone and/or an increase in sex hormone biding globulin (SHBG). Furthermore, high prolactin hormone levels may suggest a pituitary tumor that may be causing a decrease in testosterone production.
It is important that your doctor measure hormones in the HPGA cascade to diagnose what kind of hypogonadism you have. The most common kind of hypogonadism presents low testosterone with normal or elevated FSH and LH levels, which indicates that your testicles are not responding to the signals of both LH and FSH. This is what is called primary hypogonadism.
There are several reasons that testosterone levels may be low:
- Too much testosterone is being converted into estrogen through the activity of the aromatase enzyme, and/or the liver is failing to remove excess estrogen. This could be caused by heavy alcohol intake or the effect of some medications on estrogen clearance in the liver.
- Too much free testosterone is being bound by SHBG. This would be especially apparent if a male’s total testosterone level is in the high reference range but his free testosterone (unbound) level is low. As previously mentioned, aging and illness increase SHBG.
- The pituitary gland which controls testosterone production through the production of LH, is not secreting enough LH to stimulate production of testosterone by the testicles. In this case, total testosterone would be low.
- The hypothalamus is not functioning properly. LH levels of less than 2 ng/mL suggest a lesion in this part of the HPGA.
- The testicles have lost their ability to produce testosterone, despite adequate amounts of LH. In this case, the level of LH would be high (greater than 10ng/mL) despite a low testosterone level.
- Dehydroepiandrosterone (DHEA) level is abnormally low. DHEA is a hormone produced by the adrenal glands that has a lot of the same benefits as testosterone. It also is a precursor to testosterone in women.
- Disease or infections.
- Street drugs, prescription or over-the-counter medications (more on this later).
- Foods (more on this later).
- Lab error.
- High prolactin levels, which may indicate the presence of a pituitary tumor that impairs production of hormones that tell your testicles to produce testosterone (rare condition but worth mentioning!)
- Defects in genes that affect LH and FSH production.
Diagnosis of Testosterone Deficiency
Lab work will play an important role in diagnosing hypogonadism. Your doctor will likely check your total testosterone and your free testosterone levels. There are some things you should know about these tests, including what they represent and when they should be done.A “normal” total testosterone scale from most laboratories is generally between 300 and 1,000 ng/dL for men and between 25 and a round 90 ng/dL for women. The normal range from most laboratories for free testosterone usually is between 3.06 and 24 ng/dL for men and between 0.09 and 1.28 ng/dL for women.
As mentioned earlier, free testosterone is not bound to blood carrier proteins, so it is “free” to diffuse readily into cells where it signals them to adjust their activity. Some studies report that free testosterone may be a better indicator for quality of life and lean body mass, but there are some conflicting studies on this issue.
Since aging and illness can increase SHBG, which can attach to testosterone to impair its effectiveness, it becomes more important to test for free testosterone if you are older or being challenged by illness.
Many doctors treat their patients according to hypogonadism symptoms regardless of what their testosterone blood levels are. They use optimal ranges of 500 to 1,000 ng/dL for total testosterone and 100 to 200 ng/dL for free testosterone for men and 50 to 100 ng/dL for total testosterone and 1to 2 ng/dL for free testosterone for women. Table 2 shows the reference ranges for free testosterone according to age in men.

Figure 5. Testosterone decreases as we age (Courtesy of Medscape)As you can see in Figure 5, testosterone decreases as we age. This decline is due to many factors that get in the way of retaining a healthy testosterone blood level. Among them are inflammatory states caused by being overweight, diet, medications, alcohol and street drug abuse, stress, lack of adequate sleep, and problems with how the body uses carbohydrates for energy (due to impaired function of the blood sugar controlling hormone insulin). Some experts also think that our own bodies are slowly turning down their engines to get ready for a slower pace and eventual death. However, many physicians in the aging field have now begun to believe that we can grow older while keeping our strength, sexual function, lean tissue, and cognitive function so that we have more “disability-free” years.
Testosterone levels can vary throughout the day. Young and adult men tend to have higher testosterone levels in the morning than in the evening (see Figure 6). This variation is less evident as men age, however. This fact may explain why it’s not uncommon for men to have morning erections.
Some physicians recommend doing hormone testing in the morning on an empty stomach, as many things can affect free testosterone measurements, including diet. Elevated insulin caused by eating carbohydrates, for instance, can increase free testosterone levels by reducing plasma levels of SHBG.
Some doctors tend to test this hormone in the late afternoon since the levels may be lower then. In my opinion, it is not practical to restrict testing of this hormone to early morning times and in a fasting state since intraday
fluctuations are not that great in men over 30 and it may be equal to laboratory variability.
Figure 6. Variations in testosterone blood levels during the day for young and older men.
Normal values may vary from lab to lab depending on what reference range they use. Your doctor will have your test results in one to two days. Depending on the country, ranges are in nanograms per deciliter (usually in the United States) or nanomoles per liter (Europe and other countries). The conversion factor is:
Testosterone in ng/dL × 0.035 = Testosterone in nanomolars per liter
Table 2. Laboratory Ranges and Codes (courtesy of LabCorp)
Total Testosterone for Males
Age
7 months to 9 years
Less than 30 ng/dL (< 1.04 nmol/L)
10–13 years
1–619 ng/dL (0.04–21.48 nmol/L)
14–15 years
100–540 ng/dL (3.47–18.74 nmol/L)
16–19 years
200–970 ng/dL (6.94–33.66 nmol/L)
20–39 years
270–1,080 ng/dL (9.00–37.48 nmol/L)
40–59 years
350–890 ng/dL (12.15–30.88 nmol/ L)
60 years and older
350–720 ng/dL (12.15–24.98 nmol/L)
Reference Intervals for Free Testosterone
Age
20–29 years old
9.3–26.5 picograms/mililiter (pg/mL)
30–39 years old
8.7–25.1 pg/mL
40–49 years old
6.8–21.5 pg/mL
50–59 years old
7.2–24.0 pg/mL
Testosterone Formulations
In theory testosterone replacement should approximate the body’s own natural production of the hormone. The average male produces 4 to 7 mg of testosterone a day with plasma levels in early morning and lower levels in the evening. Women produce around a 12th of those rates.Testosterone replacement is usually a life-long commitment. It is a decision that should not be made without a discussion with your health care provider. Starting and stopping testosterone can have negative effects on someone’s quality of life (more on this topic later).
There are testosterone replacement products that require daily dosing (orals, buccal, and gels), once a week or two weeks dosing (injections), and once every three- to four-month dosing (long-acting testosterone undecanoate injections (not yet approved in the United States as of 2010) or testosterone pellets).
Males who are hypogonadal can be given continuous testosterone replacement therapy in a wide assortment of ways. These include:
- Oral capsules
- Testosterone injections
- Transdermal (absorbed through the skin) testosterone cream or gel
- Transdermal testosterone patch
- Buccal (sublingual and gum adherent)
- Pellets (that are implanted subcutaneously)
—————————————————————————
About the Author:
Nelson Vergel is the author of “Testosterone: A Man’s Guide” and co-author of the book “Built to Survive”, thefounder of the Body Positive Wellness Clinic in Houston, and an expert speaker on exercise, nutrition, testosteronereplacement, metabolism , sexual function and therapies to increase lean body mass and decrease fat. He hasprovided over 500 lectures in the past 15 years in the U.S. and overseas. He provides patient-friendly informationaccessible to all, no matter of their knowledge base. More on Nelson Vergel atwww.nelsonvergel.com




COMMENTS